
Mission Creep
When and how did "Protect the Vulnerable" become "Everyone should get Vaccinated"?


This question has been nagging me, especially since my post, Noble Lies and Shady Deals, about the massive Covid-19 vaccine orders the Germany goverment contracted in winter 20/21: just when did public health policy shift from vaccinating the elderly and vulnerable to getting as many people “jabbed” as possible? Before, after, or at the same time as governments were placing vaccine orders far in excess of their populations’ requirements?
The UK-based “The Health Foundation” published a helpful online explanatory guide 19 December 2020 entitled, “The COVID-19 vaccine: who gets it first?”, in which they describe the UK authorities’ vaccination campaign. It explores the trade-offs that government had to consider in deciding which groups get the vaccine first and it was based on the latest advice from the Joint Committee on Vaccination and Immunisation (JCVI)1: (all emphasis mine)
The NHS’s vaccination campaign hopefully marks the beginning of the end of the pandemic. However, as vaccines will be in short supply for months, government has had to make decisions about who to vaccinate first.
The German Robert Koch Institute (RKI equivalent to American CDC) similarly stated in it’s press release2 on 17 December 2020:
As only a limited amount of vaccine doses are available, these should be used in accordance with the recommendations of the STIKO (Standing Vaccine Commission) in order to reduce the number of severe courses of the disease and deaths as soon as possible.
I will return to this first point of “short supply” to address whether this suggests there may always have been a plan to vaccinate everyone and initial supply was the constraining factor.
Preventing Mortality or Transmission?
Again from the UK-based Health foundation:
Vaccines can do two things. First, they can protect vaccinated individuals by reducing their risk of catching the virus or developing severe disease thus preventing deaths. Second, they can also protect societies, including unvaccinated individuals, by reducing transmission.
This is the crux of the initial vaccine rollout discussion detailed in the JVCI document: direct (mortality) protection vs indirect (transmission) protection. Note, direct protection is at the level of the individual, whereas indirect protection is at the societal level. Therefore, the first, direct protection is of greatest interest for you and your doctor advising you, and the second, indirect societal protection, is of greatest interest to public health officials advising governments.
The two levels involve different and seperate risk-benefit calculations. Remember, a doctor’s first responsibility is to their patient (not the government!) and the Hippocratic Oath declares “first do no harm” so these two levels can be in conflict, i.e. what your doctor considers best for you individually may not be what public health thinks is best for society. It is also no secret there are many precedents of authoritarian regimes seeking to justify repression or coercion in the name of protection and security of the nation or “the people”.
The current approach [December 2020] prioritises reducing mortality over reducing transmission and therefore targets vaccination at those most likely to die as a result of COVID-19. Because age is the primary predictor of COVID-19 mortality, this means mainly targeting older people.
Numbers Needed to Vaccinate
Without explicitly mentioning NNTV (Numbers Needed To Vaccinate3), which in turn is based on the Absolute Risk Reduction (ARR) - two concepts hidden by the more spectacular claims of Relative Risk Reduction (RRR) touted by the vaccine manufacturers - the Heart Foundacion continues with the following easily understandable example:
It would be necessary to vaccinate around 32 times more 60–64 year olds than those older than 90 years old to save a life, or six times as many to save one year of life. Front-line health and social care workers and the clinically vulnerable will also be vaccinated.
Leaving aside the accuracy of the figures presented, the principle is important: there was at an official level a recognition of diminishing returns involved as you vaccinate down through the vulnerable age groups. The JVCI report, “Joint Committee on Vaccination and Immunisation: advice on priority groups for COVID-19 vaccination, 30 December 2020”, openly stated:
Current evidence strongly indicates that the single greatest risk of mortality from COVID-19 is increasing age and that the risk increases exponentially with age...
Ahh there’s that word again, “exponentially”. Remember the days when your colleague or neighbour became an overnight expert on explaining exponential growth of pandemics using facile analogies from their favourite MSM science-explainer, like rice grains on a chess board or some other such silliness completely neglecting real world self-limiting properties of complex inter-connected systems? Anway, in this instance, exponential means the chances of dying from Covid-19 became vanishingly small as you descended down through the age groups of younger healthy individuals.
Mortality - Top Priority
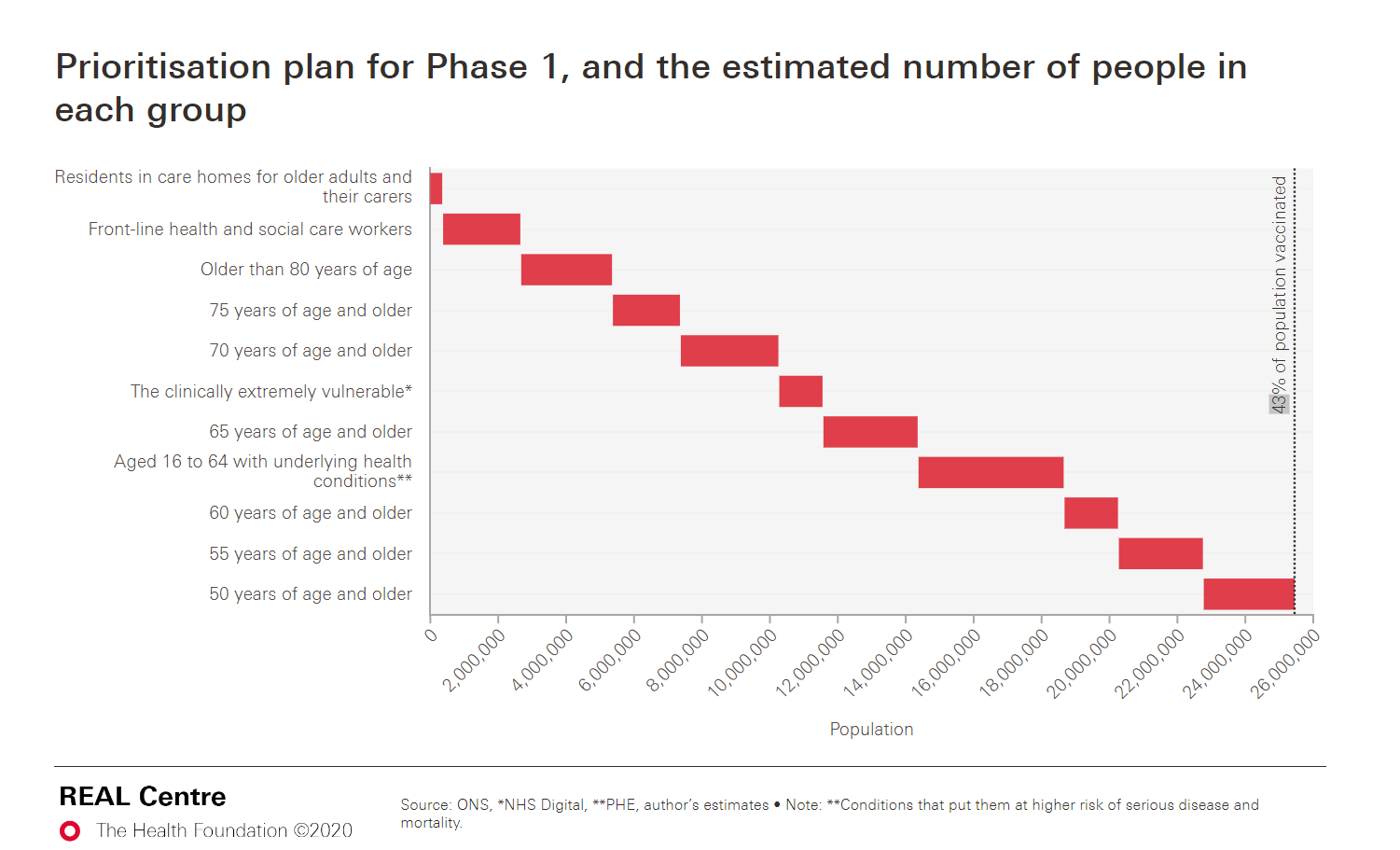
Referring to the prioritised groups in the graphic below and the estimated number of people in those groups the JVCI stated:
It is estimated that taken together, these groups represent around 99% of preventable mortality from COVID-19.
Think about that: 99% of preventable deaths. Direct, personal protection of the vaccines was estimated to prevent 99% of deaths if administered to the older 50+ and more vulnerable groups. Again, I am not arguing for this policy nor it’s accuracy (it is afterall based on ~95% vaccine efficacy), rather I want to highlight that at an official level this was the thinking. So why on earth did they continue to keep pushing through the younger less vulnerable cohorts? If the authorities truly believed the manufacturer claims of the vaccine efficacy against death and serious illness, what was the purpose in expanding the vaccine campaign to general populations?

Herd Immunity - Out of Reach
Herd immunity was being talked about early on and some public health officials and governments may naively have been chasing the unattainable goal of eradicating Covid but already there was much disagreement amongst many in the scientific community. An article in Nature Magazine4 appearing 18 March 2021 stated:
“The key to herd immunity is that, even if a person becomes infected, there are too few susceptible hosts around to maintain transmission — those who have been vaccinated or have already had the infection cannot contract and spread the virus.”

The article is full of qoutes from various scientists which are often contradictory.
“Herd immunity is only relevant if we have a transmission-blocking vaccine. If we don’t, then the only way to get herd immunity in the population is to give everyone the vaccine,” says Shweta Bansal, a mathematical biologist at Georgetown University in Washington DC.
What? Herd immunity only works if the vaccines work well, if they don’t, then everybody has to get vaccinated? And this is before we even get to the topic of variants and the rapidly mutating nature of Sarbecoronaviruses:
There’s another problem to contend with as immunity grows in a population, Ferrari says. Higher rates of immunity can create selective pressure, which would favour variants that are able to infect people who have been immunized. Vaccinating quickly and thoroughly can prevent a new variant from gaining a foothold.
Let’s just say the jury was out on herd immunity, there was certainly no scientific consensus and governments must have been aware of this. [See IMPORTANT UPDATE at end with link to Igor Chudov’s new post!]
Transmission - Where’s the Data?
Even if we accept expanding vaccination campaigns to non vulnerable groups was an effort to reduce overall transmission and prevalence of infections within the general population once enough vaccines were available, where was the data to justify such an approach? The following may surprise those who regarded it as a “gotcha” moment when Pfizer admitted to the European Parliament that it had not tested the ability of its COVID-19 vaccine to prevent transmission of the virus before it entered the market. But while it was not widely propogated by MSM in early 2021 it certainly was not news within public health circles - from the same JVCI report end of 2020:
However, at this time there is no data on the size of the effect of COVID-19 vaccines on transmission. Evidence is expected to accrue during the course of the vaccine programme, and until that time the committee is not in a position to advise vaccination solely on the basis of indirect protection.
There was no data in December 2020. They simply did not and could not know.
Wider use of COVID-19 vaccines will provide a better understanding of whether they can prevent infection and onward transmission in the population. Data on vaccine impact on transmission, along with data on vaccine safety and effectiveness, will potentially allow for consideration of vaccination across the rest of the population.
They were going to wait on real world population-level data to assess the efficacy against transmission and this would potentially allow for consideration of vaccination acfross the rest of the population. This language is very circumspect and related back to the very first point about supply constraints would suggest, “no”: supply constraints were not the main stumbling block; it was “lack of data” and the JCVI weren’t making any promises. So I guess they got that missing data because we all know the vaccine campaigns did expand and in many countries became mandates, right?
Germany authorities echoed this in their press release, 12 Dec 2020. Here the RKI hints at the desire to vaccinate everyone but also concedes they just didn’t know the effectiveness against transmission:
In the medium term, the goal is to be able to offer COVID-19 vaccination to everyone. “In order to significantly mitigate the spread of SARS-CoV-2, a majority of the population must develop immunity against the virus”, said Prof. Lothar H. Wieler, President of the Robert Koch Institute [equivalent of Fauci in Germany - also quitting start of 2023]. “Vaccination with safe and effective vaccines therefore makes a critical contribution to fighting the pandemic”. However, it will take some time until a relevant proportion of the population is protected from COVID-19 by vaccination. Furthermore it is not yet clear to what extent the vaccination also prevents or at least reduces transmissions of the virus.
Show me the data!
A couple months into the rollout in March 2021, the UK’s COVID-19 Vaccine Surveillance Strategy5 paper was published and under point 5, “Vaccine Effectiveness” we find:
Clinical trials are also typically powered for a primary endpoint of virologically confirmed symptomatic disease within a relatively short followup period so that effective vaccines can be introduced as rapidly as possible. Nevertheless, understanding the effectiveness against different end points (such as disease severity and onwards transmission), effectiveness in different subgroups of the population and understanding the duration of effectiveness are equally important in decision making around which vaccines should be implemented as the programme evolves, who they should be offered to and whether booster doses are required.
In March, after a couple months of actively rolling out the vaccines, they were still talking about a developing situation with regard to duration of effectiveness, with regard to who (younger age groups?) should receive them, and they were already considering if boosters would be required.
Effect of vaccination on transmissibility
As well as understanding the impact of vaccination on disease outcomes and infection it is also important to understand whether it reduces the risk of onwards transmission. This will inform policy decisions around whether to prioritise vaccination of those with worse outcomes or those who transmit more.
Note this language in this excerpt (from same document in March) shows they still wanted to understand whether it reduces the risk of onwards transmission - they did still did not reliably know! Meanwhile there had been strong take up in the older age groups in the UK and public health started to considered everyone over 18 eligible.
Fast forward to UK’s COVID-19 vaccine surveillance report - Week 396 in September:
Effectiveness against transmission
As described above, several studies have provided evidence that vaccines are effective at preventing infection. Uninfected individuals cannot transmit; therefore, the vaccines are also effective at preventing transmission. Data from Scotland has also shown that household contacts of vaccinated healthcare workers are at reduced risk of becoming a case, which is in line with the studies on infection (16). There may be additional benefit, beyond that due to prevention of infection, if some of those individuals who become infected despite vaccination are also at a reduced risk of transmitting (for example, because of reduced duration or level of viral shedding).
Little evidence - Low confidence
In September they still didn’t know if breakthrough vaccinees were less likely to infect others. However, they inferred indirect protection because uninfected people cannot transmit and the vaccines had demonstrated some protection (limited) against infection, at least in early 2021:

Interestingly, effectiveness against transmission is not even listed and effectiveness against infection (60%~85% depending on vaccine) is categorised as low confidence meaning “little evidence is available at present and results are inconclusive”. So by September although they were already encouraging younger cohorts to get vaccinated they had little evidence to support this and what little they had was considered inconclusive that it was proabably better than 50% effective at preventing infection? That’s a whole lot of maybe three quarters of a year after rollout.
Meanwhile from RKI in Germany, 23 September 20217:
Postmarketing and Real-Life Studies have show that viral shedding from individuals infected with SARS-CoV-2 despite a completed vaccination series is reduced and therefore the risk of transmission is significantly reduced. However, it must be assumed that people can become symptomatically or asymptomatically infected after relevant exposure despite vaccination and can emit SARS-CoV-2 in the process.
So, we had reached end of September 2021, breakthroughs were a recognised phenomenon, and it was accepted that vaccinated can be spreaders. Somehow the German RKI could claim significantly reduced transmission based on “real-life studies” and yet fail to list or link a single supporting study in the same document? [Edit: as pointed out by cm27874, mere statistical significance is meant here] Just how did we progress from that to vaccine-status discrmination and mandates?
Israel - a “sort of laboratory”
In early September Philip Dormitzer, the chief scientific officer at Pfizer, made the following comments to a Zoom gathering of academics as reported in the Times of Israel:
“Early in the pandemic we established a relationship with the Israeli Ministry of Health where they used exclusively the Pfizer vaccine and then monitored it very closely,” Dormitzer told the gathering, “so we had a sort of laboratory where we could see the effect.”
He added that Israel “immunized a very high proportion of the population very early — so it’s been a way that we can almost look ahead: What we see happening in Israel happens again in the US a couple months later.”
Well, what did we see happening in Israel that would be expected to later happen in the rest of the world?
Waning Efficacy - a disappearing act
At the end of July, the Israeli president announced the booster campaign initially for over 60’s who had received their last dose at least 5 months previously. The reason? The israeli authorities were noticing a higher incidence in Covid cases amongst those vaccinated earlier (longer ago). From the New York Times8, 23 July 2021:
Analyzing the government’s national health statistics, researchers estimated that the Pfizer shot was just 39 percent effective against preventing infection in the country in late June and early July, compared with 95 percent from January to early April. In both time periods, however, the shot was more than 90 percent effective in preventing severe disease.
That’s less than 50%, at those rates it’s like flipping a rigged coin to see if your vaccine protects you from infection.
What about Natural Immunity?
Pfizer’s Israel laboratory also provided insight into vaccine efficacy versus infection conferred immunity. From another article in Nature Magazine in late August ‘21, entitled “Having SARS-CoV-2 once confers much greater immunity than a vaccine - but vaccination remains vital9” [the doublethink is astounding]. The lede: “Israelis who had an infection were more protected against the Delta coronavirus variant than those who had an already highly effective COVID-19 vaccine.” Highly effective = less effective than infection-conferred protection.

Long-Covid?
Finally, a growing narrative in 2021 evolved around the risk of so-called Long-Covid, otherwise known as post-acute sequelae of COVID-19 (PASC). It is important to note that Long COVID had been observed as a consequence of both mild and severe infection so the extent to which the vaccines could provide any direct protection (as opposed to indirect protection via any effectiveness against infection or severe infection) was potentially an extra selling point for the vaccine promoters.
People with Long-Covid were left out of the original vaccine trial studies so as with transmission, public health authorities would have to wait and see as the real world data rolled in. In June 2021 an article in Nature, “The four most urgent questions about long COVID10” concluded:
… there is the question of what part COVID-19 vaccines might play. Although many of them prevent death and severe illness, scientists do not yet know whether they prevent long COVID.
What about the impact of vaccines in people who already have long COVID? A UK survey of more than 800 people with long COVID, which has not been peer reviewed, reported in May that 57% saw an overall improvement in their symptoms, 24% no change and 19% a deterioration after their first dose of vaccine.
How do you like those odds? Then consider how mandates forced many to roll that dice. And I don’t know whether to laugh or to cry at the statement from Athena Akrami, a neuroscientist at University College London investigating Long-Covid:
In April[2021], Akrami’s team launched a systematic survey to shed more light. “People need to get vaccinated to come out of the pandemic, but we need to first address their concern of whether the vaccine is going to help, or not harm, or [be] harmful.”
A recent meta-analysis11 from December 2022 of six studies estimates that one dose or more of COVID-19 vaccine is 29% effective against symptoms persisting for at least 3 weeks after infection, or long COVID. So two years after the rollout under emergency/conditional use authorisations the vaccines are demonstrating inadequate effectiveness against Long-Covid to ever achieve a normal authorisation.
Summary
Let’s take a step back to summarise what I have covered so far, and it’s by no means exhaustive:
Majority of populations (young and healthy) were not at high risk
Lack of data around vaccine protection against transmission
Herd immunity was disputed and even considered unattainable [see UPDATE]
Mass-vaccination programmes can create selective pressure for new escape variants
Vaccine protection was limited and rapidly waning
Natural (infection-conferred) immunity was superior to vaccination only
Any effectiveness against Long-Covid was very poorly understood
And yet the German government still pushed ahead, doubling-down by ordering 100’s of millions more doses of an experimental gene therapy product in election week September 2021. They introduced discriminatory laws and created different classes of citizens based on their “vaccine status”. They introduced vaccine mandates for workers in healthcare workplaces, and they tried to introduce vaccine mandates for the entire adult population in spring 2022.
I thought understanding when authorites knew how well the vaccines did (not) provide effective protection against transmission would be critical to assessing motivations behind vaccine passports and mandates and perhaps identifying the role financial considerations or sunk costs played in those policy decisions. I have tried to give the benefit of the doubt, but it’s doesn’t look good. In a follow-up post I plan to go down the rabbit hole of the 2009 Swine Flu “Epidemic”.
[UPDATE: Igor Chudov has posted an excellent piece featuring a newly published study, “Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses”. Seems kinda incriminating for one of the authors, a certain Mr Anthony Fauci:

Bonus Quotes:
Two statements twelve months apart. First from Dr “I am the science” Fauci of the american CDC in May 2021: -
“When you get vaccinated, you not only protect your own health and that of the family but also you contribute to the community health by preventing the spread of the virus throughout the community… In other words, you become a dead end to the virus. And when there are a lot of dead ends around, the virus is not going to go anywhere. And that’s when you get a point that you have a markedly diminished rate of infection in the community.”
Second, from Bill Gates, the world’s biggest private supporter, financer, and promoter of vaccines, at the World Economic Forum during a panel entitled “Preparing for the Next Pandemic” on 24 May 2022: -
“Today, you know, the vaccines have saved millions of lives [Witzbold: based on models ;) ], but they don't have much in the way of duration and they're not, they’re NOT good at infection blocking.”
“The idea of checking if people are vaccinated - you know, if you have breakthrough infections… what’s the point?”
As ever, I appreciate any and all feedback - let me know if you think I have missed something! And please share my articles if you think others would appreciate them:

Good post, Witzbold - thanks. I did a similar analysis of what happened between Nov 2020 and Jan 2021: https://open.substack.com/pub/alexstarling77/p/tina-turned - "There Is No Alternative" (to universal rollout) was allowed to become gospel, at least in part due to suppression of rational discussion and cost/benefit analysis.
I also thought that this comment in Dec 2022 from one who celebrated "extraordinary vaccine success" in Jan 2021 is kind of telling:
“The entire population was vaccinated or offered the vaccine, which now looks like a terrible idea when there were deaths among young people who really had no need to be vaccinated. They were not at risk from Covid. The mantra was it limited transmission. We hear less about that now. Parliament was shut down. Government colluded with social media giants to suppress legitimate questions about the origin of the virus and all manner of other policy debates”. Ref:
https://reaction.life/time-to-talk-about-covid-mistakes/ ... what a difference 23 months make! It is still - to me - unbelievable that so many people's survival instinct didn't kick in earlier.